Q: What tubes can I use to draw a Type and Screen?
Q: If I don't have any pink tubes, can I use another color tube?
Q: Why is blood bank changing to Pink Tubes?
Q: What tube should I use for Pediatrics?
Q: What is the minimum amount of blood for adults and pediatric specimens?
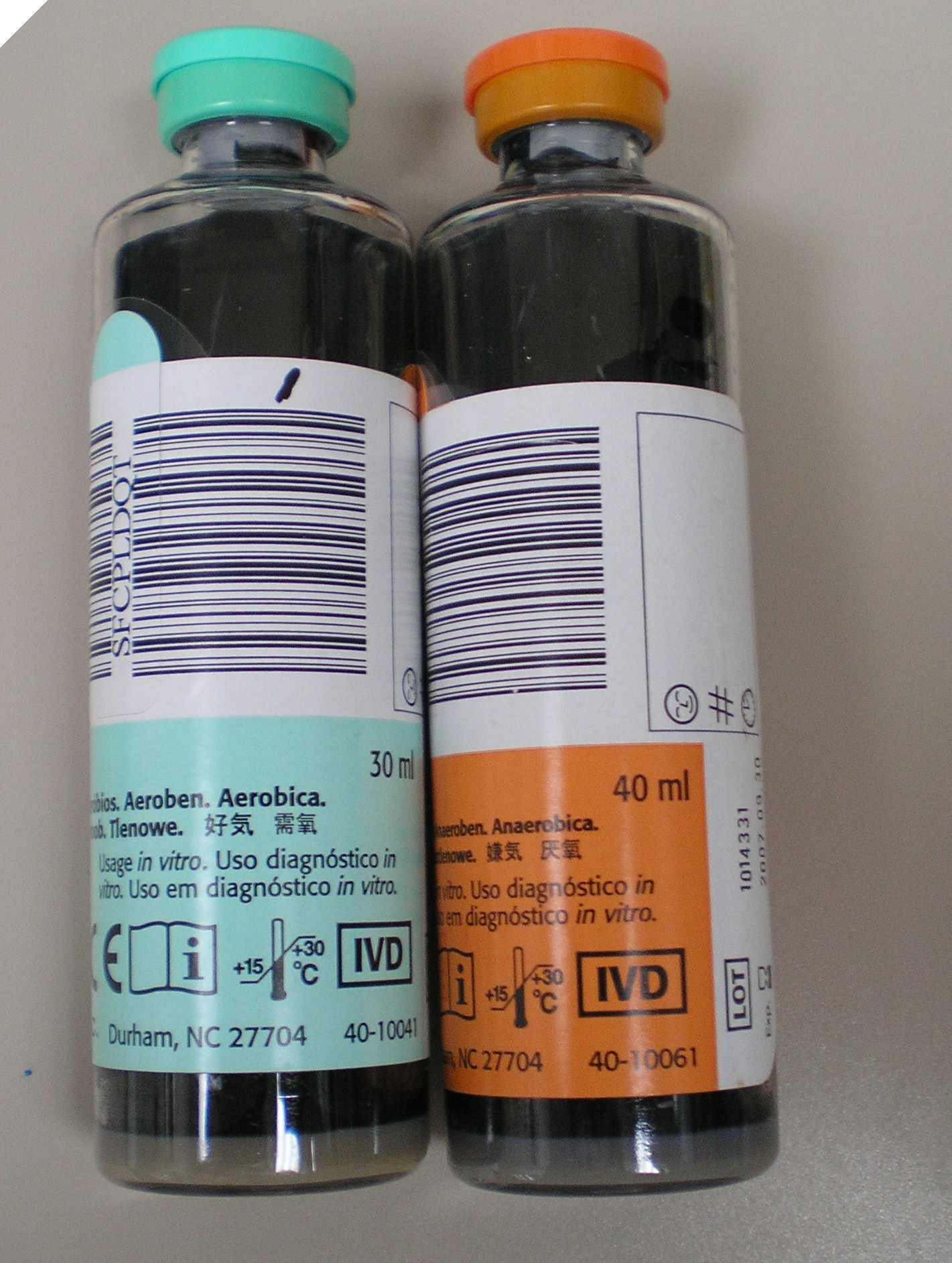
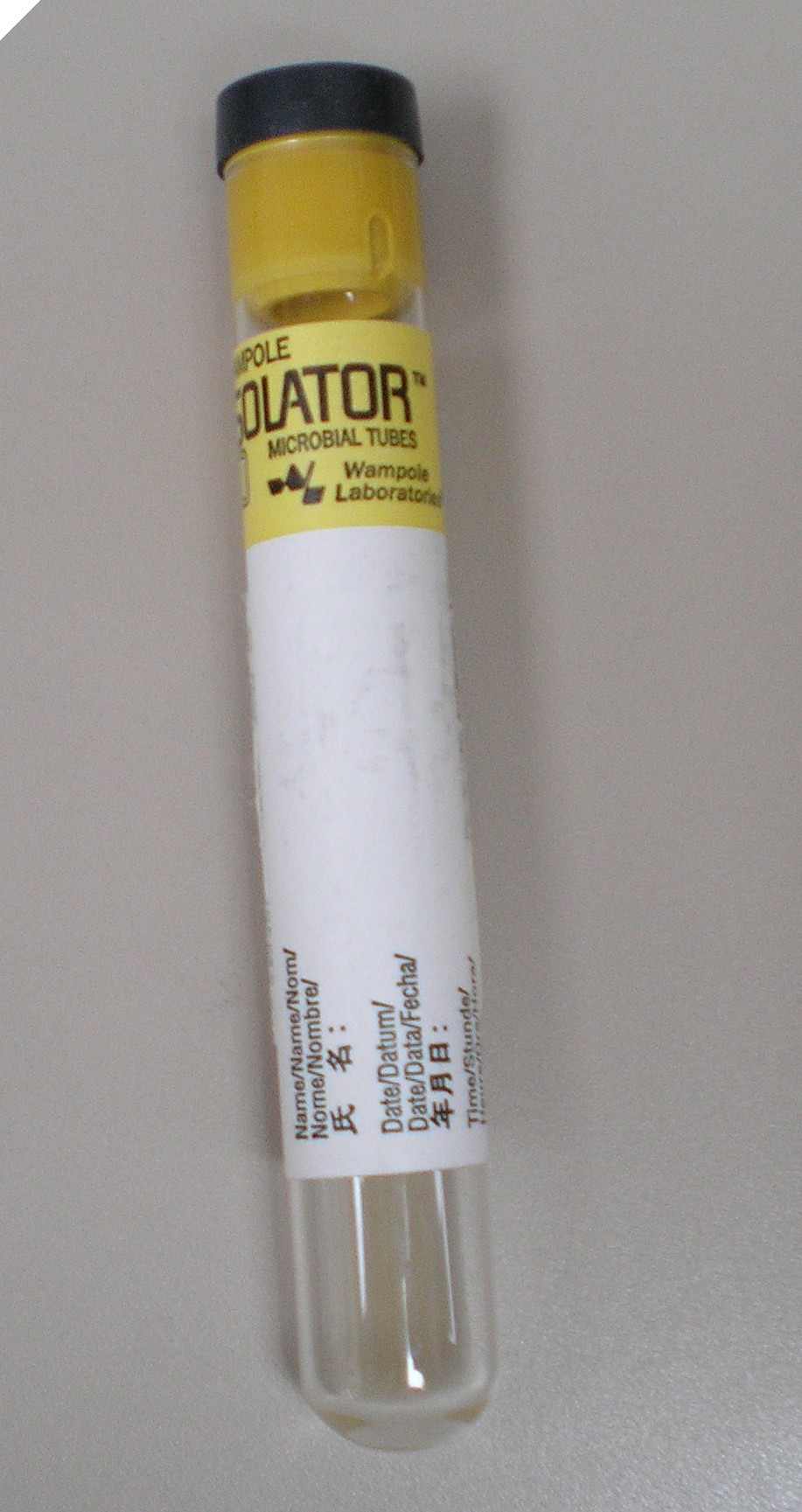
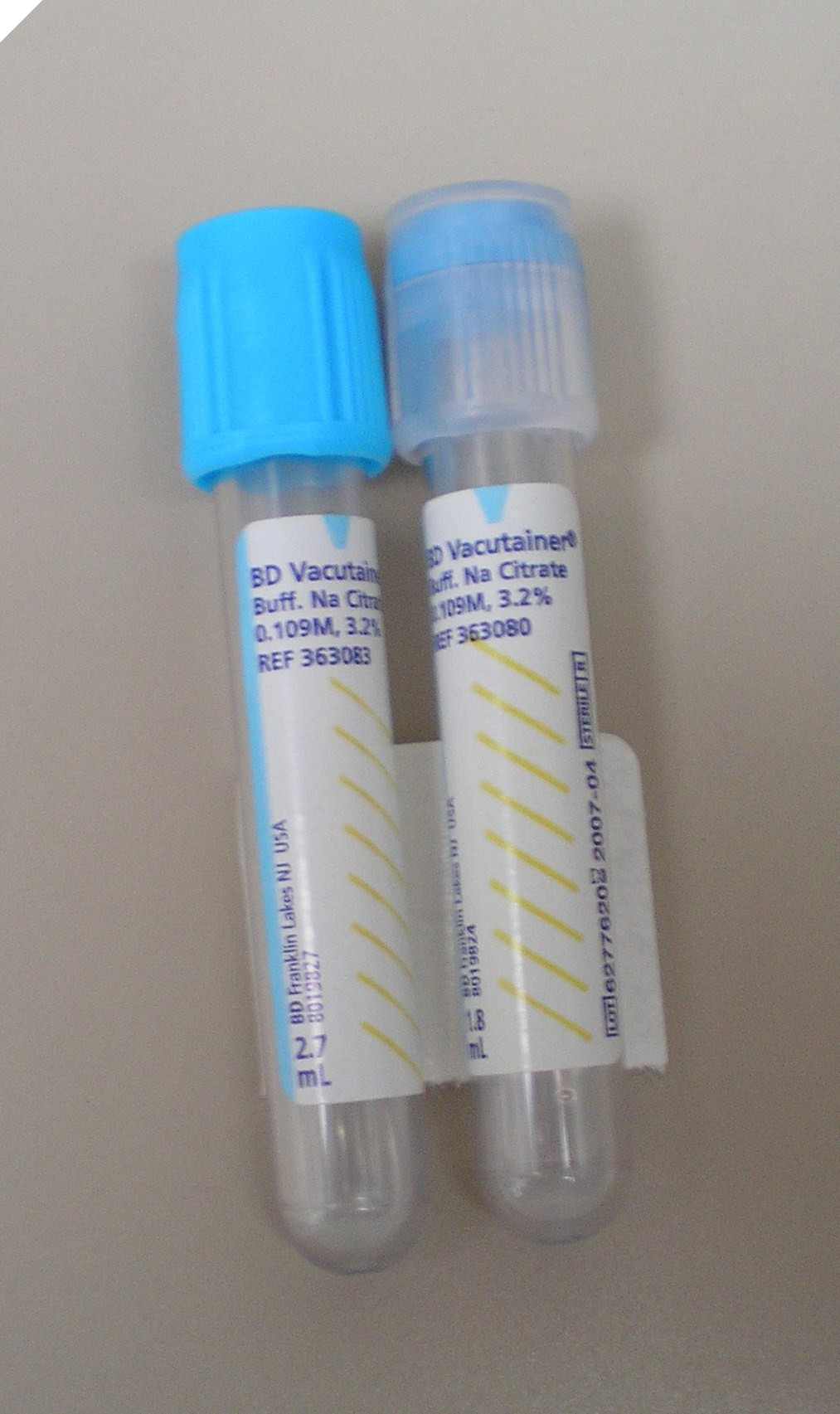
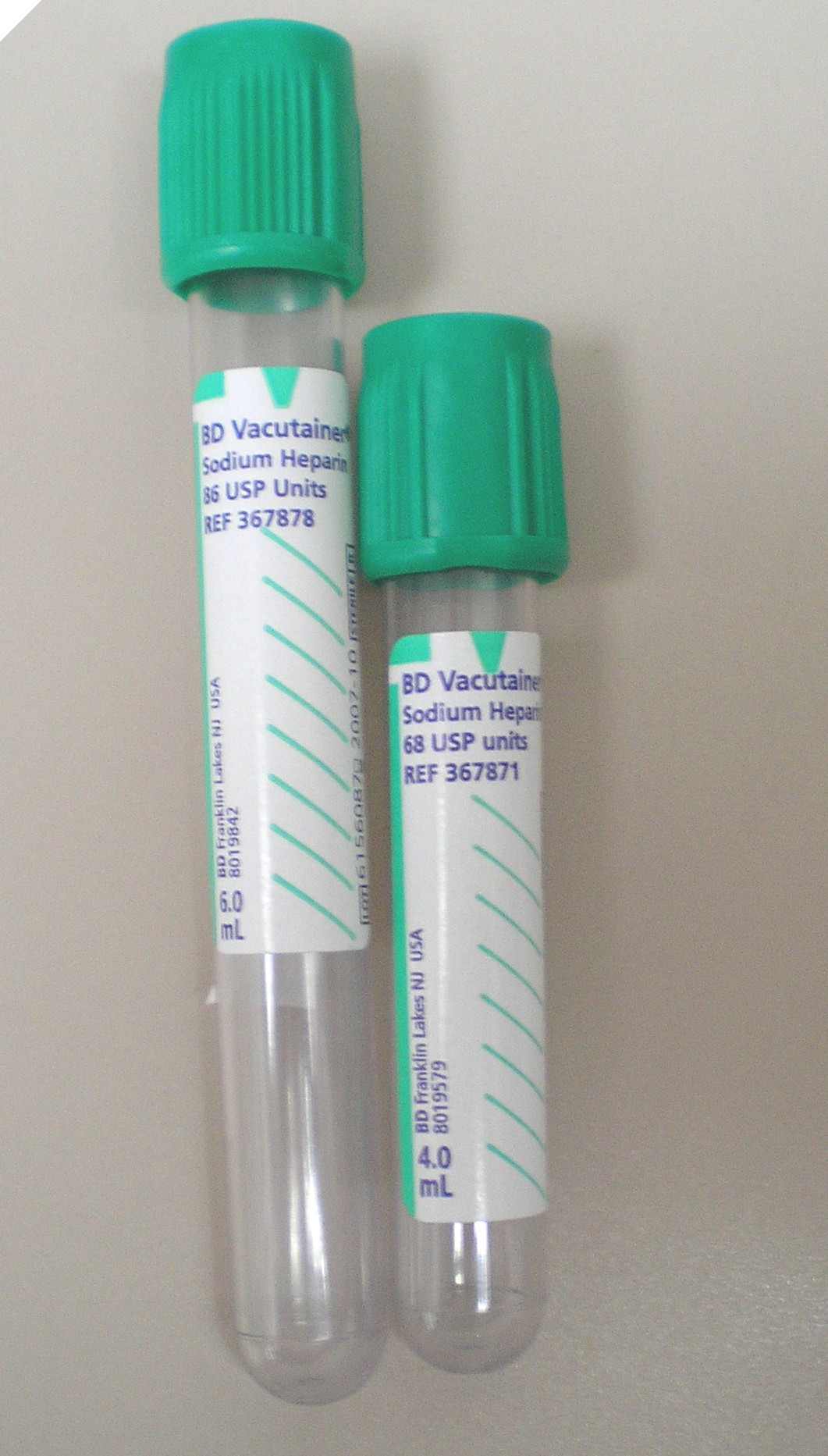
Q: In what order should I draw specimens?
Q: How do I label a tube?
Q: How long is a type and screen good?
Q: Can I draw a blood specimen while the patient is being transfused?
Q: Why must I throw away the first tube when collecting a blood specimen for laboratory testing from a catheter or central line?
Q: Can Alaris infusion pumps be used with blood components?
Q: How many products can be infused through a line/tubing setup?
Q: What blood products need filters?
Q: How long can Red Blood Cells and Plasma be outside of a blood bank refrigerator?
Q: How long can a blood component hang?
Q: How frequently should vital signs be taken during a transfusion?
Q: Can we give blood components with an automated pump (example Alaris, IVAC or ABBOTT pump)?
Q: How fast can we give blood components? Should Platelets be Transfused Slowly?
Q: What is the smallest needle we can use to transfuse blood components?
Q: If a patient has a fever, can I transfuse blood components?
Q: What is the policy for transporting patients with blood hanging?
Q: Can we give Rh positive components to Rh negative patients?
Q: How does a split product read on the form?
Q: If a blood product has been double checked at the bedside and it is removed from the bedside, do I need to double check the blood again when the blood is brought back to the patient's bedside?
Q: Can I transfuse different products through regular blood tubing?
Q: How often should I change blood filters?
Q: Can I mix different products in the same set at the same time?
Q: Can a PALL white blood cell removal filter be used with an infusion pump?
Q: If a product outdates while hanging, is it still good? For how long?
Q: What components need to be double checked before transfusion?
Q: When do you use a Pall leukocyte removal filter?
Q: If I use a Pall leukocyte-removal filter do I need to use a blood administration tubing set as well?
Q: Is there any written information on how staff could determine how long to run a unit of Red Blood cells for kids? I see adult tranfusoin flow rates in the blood information.
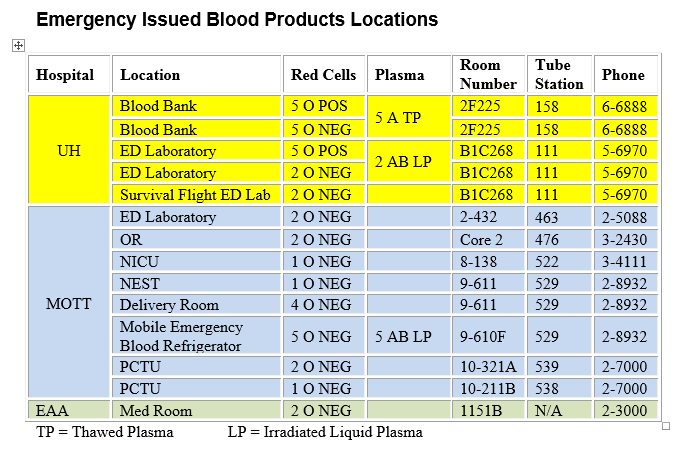
Q: How do I handle an emergency transfusion?
Q: How is albumin transfused?
Q: Can a double lumen catheter be used to transfuse blood components?
Q: What are my responsibilities when caring for a patient with a suspected transfusion reaction?
Q: What is a febrile transfusion reaction?
Q: What is an urticarial reaction?
Q: What is an acute hemolytic reaction?
Q: What is a Delayed Hemolytic Transfusion reaction?
Q: Who should obtain consent for blood transfusion?
Q: Can a nurse or other health care professional sign as the witness on the Informed Consent form?
Q: Where can I get a copy of the Consent to Receive Blood Transfusion or the Refusal for treatment forms?
Q: Is there a time limit on the Consent for Transfusion?
Q: Should the patient carry a copy of the Consent form if the patient is being tranfused on an outpatient basis?
Q: When should a post transfusion sample be collected to monitor the transfusion of Red Blood Cells and Platelets?
Q: What should I do if a patient shows me a card from the Blood Bank or Transfusion Service of an outside institution saying the patient has antibodies or problems with blood transfusions?
Q: Where can I find more information about RhoGAM®?
Q: The unit of Red Blood Cells is labeled as outdating today. What time today does it outdate?
Q: Are there ay blood substitutes that can be used for patient who refuse blood transfusion?
Q: Do you perform paternity testing?
Q: Do you have a cord blood bank for future infusions?
 ON THE COVER
ON THE COVER
Breast team reviewing a patient's slide. (From left to right) Ghassan Allo, Fellow; Laura Walters, Clinical Lecturer; Celina Kleer, Professor. See Article |
newsletter
INSIDE PATHOLOGYAbout Our NewsletterInside Pathology is an newsletter published by the Chairman's Office to bring news and updates from inside the department's research and to become familiar with those leading it. It is our hope that those who read it will enjoy hearing about those new and familiar, and perhaps help in furthering our research. CONTENTS
|
 ON THE COVER
ON THE COVER
Autopsy Technician draws blood while working in the Wayne County morgue. See Article |
newsletter
INSIDE PATHOLOGYAbout Our NewsletterInside Pathology is an newsletter published by the Chairman's Office to bring news and updates from inside the department's research and to become familiar with those leading it. It is our hope that those who read it will enjoy hearing about those new and familiar, and perhaps help in furthering our research. CONTENTS
|
 ON THE COVER
ON THE COVER
Dr. Sriram Venneti, MD, PhD and Postdoctoral Fellow, Chan Chung, PhD investigate pediatric brain cancer. See Article |
newsletter
INSIDE PATHOLOGYAbout Our NewsletterInside Pathology is an newsletter published by the Chairman's Office to bring news and updates from inside the department's research and to become familiar with those leading it. It is our hope that those who read it will enjoy hearing about those new and familiar, and perhaps help in furthering our research. CONTENTS
|
 ON THE COVER
ON THE COVER
Director of the Neuropathology Fellowship, Dr. Sandra Camelo-Piragua serves on the Patient and Family Advisory Council. |
newsletter
INSIDE PATHOLOGYAbout Our NewsletterInside Pathology is an newsletter published by the Chairman's Office to bring news and updates from inside the department's research and to become familiar with those leading it. It is our hope that those who read it will enjoy hearing about those new and familiar, and perhaps help in furthering our research. CONTENTS
|
 ON THE COVER
ON THE COVER
Residents Ashley Bradt (left) and William Perry work at a multi-headed scope in our new facility. |
newsletter
INSIDE PATHOLOGYAbout Our NewsletterInside Pathology is an newsletter published by the Chairman's Office to bring news and updates from inside the department's research and to become familiar with those leading it. It is our hope that those who read it will enjoy hearing about those new and familiar, and perhaps help in furthering our research. CONTENTS
|
 ON THE COVER
ON THE COVER
Dr. Kristine Konopka (right) instructing residents while using a multi-headed microscope. |
newsletter
INSIDE PATHOLOGYAbout Our NewsletterInside Pathology is an newsletter published by the Chairman's Office to bring news and updates from inside the department's research and to become familiar with those leading it. It is our hope that those who read it will enjoy hearing about those new and familiar, and perhaps help in furthering our research. CONTENTS
|
 ON THE COVER
ON THE COVER
Patient specimens poised for COVID-19 PCR testing. |
newsletter
INSIDE PATHOLOGYAbout Our NewsletterInside Pathology is an newsletter published by the Chairman's Office to bring news and updates from inside the department's research and to become familiar with those leading it. It is our hope that those who read it will enjoy hearing about those new and familiar, and perhaps help in furthering our research. CONTENTS
|
 ON THE COVER
ON THE COVER
Dr. Pantanowitz demonstrates using machine learning in analyzing slides. |
newsletter
INSIDE PATHOLOGYAbout Our NewsletterInside Pathology is an newsletter published by the Chairman's Office to bring news and updates from inside the department's research and to become familiar with those leading it. It is our hope that those who read it will enjoy hearing about those new and familiar, and perhaps help in furthering our research. CONTENTS
|
 ON THE COVER
ON THE COVER
(Left to Right) Drs. Angela Wu, Laura Lamps, and Maria Westerhoff. |
newsletter
INSIDE PATHOLOGYAbout Our NewsletterInside Pathology is an newsletter published by the Chairman's Office to bring news and updates from inside the department's research and to become familiar with those leading it. It is our hope that those who read it will enjoy hearing about those new and familiar, and perhaps help in furthering our research. CONTENTS
|
 ON THE COVER
ON THE COVER
Illustration representing the various machines and processing used within our labs. |
newsletter
INSIDE PATHOLOGYAbout Our NewsletterInside Pathology is an newsletter published by the Chairman's Office to bring news and updates from inside the department's research and to become familiar with those leading it. It is our hope that those who read it will enjoy hearing about those new and familiar, and perhaps help in furthering our research. CONTENTS
|
 ON THE COVER
ON THE COVER
Rendering of the D. Dan and Betty Khn Health Care Pavilion. Credit: HOK |
newsletter
INSIDE PATHOLOGYAbout Our NewsletterInside Pathology is an newsletter published by the Chairman's Office to bring news and updates from inside the department's research and to become familiar with those leading it. It is our hope that those who read it will enjoy hearing about those new and familiar, and perhaps help in furthering our research. CONTENTS
|
MLabs, established in 1985, functions as a portal to provide pathologists, hospitals. and other reference laboratories access to the faculty, staff and laboratories of the University of Michigan Health System’s Department of Pathology. MLabs is a recognized leader for advanced molecular diagnostic testing, helpful consultants and exceptional customer service.