As the long-term Pathology Renovation and Relocation project nears completion, the opening of the new Apheresis unit in the University Hospital is one of the last major renovations to be completed.
 “This was truly a collaborative design and construction effort spanning many years,” said Christine Baker, Project Manager of the PRR project. “It was an extraordinary effort with a multi-disciplinary team, including nursing staff, faculty, designers, equipment planners, and logistics experts. The result is an optimized and beautiful patient care suite."
“This was truly a collaborative design and construction effort spanning many years,” said Christine Baker, Project Manager of the PRR project. “It was an extraordinary effort with a multi-disciplinary team, including nursing staff, faculty, designers, equipment planners, and logistics experts. The result is an optimized and beautiful patient care suite."
This space was important and exciting for faculty, staff, and patients alike as the previous Apheresis space was not ideal for such a unique patient care area.
“The results of this years-long project are stunning! Our original 7-bed unit was cramped, lacked proper storage for supplies, and offered little in the way of patient privacy,” said Michael Meade, Apheresis Service Supervisor. “Our new 10-bay unit comes with a dedicated clean supply room, an updated patient bathroom, and both patient privacy and staff line-of-sight to treatments from the central nursing station. Two thumbs up from patients, visitors, and staff!”
During the January 16, 2024, open house, Department of Pathology faculty and staff gathered to explore and enjoy the new space before the team's official moving date on January 19th and to hear Dr. Charles Parkos, Chair of the Department of Pathology express his gratitude for those who worked hard to bring the PRR project to life.
When you hear the word “pathology”, what do you think of? Do you think of a doctor in a white lab coat looking through a microscope? Or maybe a physician performing an autopsy or examining a tumor? However, often times a critical role in the pathology department is overlooked, Phlebotomy. Phlebotomy is the specialty where technicians or Phlebotomists draw and prepare blood samples for testing within the pathology labs.
In recognition of Phlebotomy Week, two members of the team, Jennifer Slater, manager for onsite phlebotomy services, and Kim Fera, clinical coordinator shared their thoughts on why phlebotomists make all the difference in patient care.
 “The phlebotomist is responsible for providing a skill and performing a procedure related to specimen collection,” said Slater. “They also are the face of the lab to a lot of patients. If you ask patients what pathology is or you ask them what the lab is, typically, someone will comment something related to a blood draw or phlebotomy or describe that type of work. I think from the lab perspective, pathology perspective, we're really important because we are the face. We are the representation of that department. We also are the start of that testing process.”
“The phlebotomist is responsible for providing a skill and performing a procedure related to specimen collection,” said Slater. “They also are the face of the lab to a lot of patients. If you ask patients what pathology is or you ask them what the lab is, typically, someone will comment something related to a blood draw or phlebotomy or describe that type of work. I think from the lab perspective, pathology perspective, we're really important because we are the face. We are the representation of that department. We also are the start of that testing process.”
Fera agreed, mentioning that without pathology and phlebotomists, patients wouldn’t be able to get better. “We really couldn't do our job without [pathologists] and they couldn't do it without us. We obtain all the blood samples and then they process it. We're one big team!”
Not only is a phlebotomist responsible for gathering samples, but also for taking care of the patients they serve. “I think that their role is not only to technically support the patient, making sure that they're providing safe and efficient care to them, but they also end up doing a lot of other things in that process. There are phlebotomists, in both inpatient and in ambulatory settings, who build really good rapport with their patients, especially those that come back to us with any kind of frequency,” Slater said.
“We talk to them. We can comfort them,” Fera mentions in relation to how for some a blood draw experience can be scary. “We need that blood to find out what is wrong so their doctors can help them get better."
 For members of the University Hospital phlebotomy team, a new change is right around the corner, one that many hope will not only help improve patient care but job satisfaction as well. As part of the department’s Pathology Relocation and Renovation project, our phlebotomists will be receiving a newly updated space, much larger than what they currently have. This new space consists of a larger cart room, office space for team leadership, break room, and conference room.
For members of the University Hospital phlebotomy team, a new change is right around the corner, one that many hope will not only help improve patient care but job satisfaction as well. As part of the department’s Pathology Relocation and Renovation project, our phlebotomists will be receiving a newly updated space, much larger than what they currently have. This new space consists of a larger cart room, office space for team leadership, break room, and conference room.
“I think giving this group an opportunity to have a refresh is important. We've been in the same room longer than I've been here and potentially longer than I've been alive,” Slater states. “The cart room is going to have a significant positive impact on our team. Our current cart room is way too small for the volume of staff and the amount of supplies that we have. I hope it means more efficient workflows, happier folks on the floors who are more excited to be at work, and all of those things will translate to the type of care they're able to provide.”
 The excitement for Fera was seen when she said “It will be like a breath of fresh air for us” noting her thoughts on how a new environment, especially one with windows, can help increase happiness and satisfaction for the team.
The excitement for Fera was seen when she said “It will be like a breath of fresh air for us” noting her thoughts on how a new environment, especially one with windows, can help increase happiness and satisfaction for the team.
“I'm hoping with this new space, we can build a stronger, healthier team.”
While Phlebotomy Week is only one moment in time, the work that our team provides is important both today and throughout the future. See more news about our phlebotomy team and PRR projects in our news section.
As part of the ongoing series of renovations of the clinical laboratories at University Hospital, the Blood Bank Laboratory — and its landmark front window — will relocate about 135 feet to the east on Sunday, June 5. 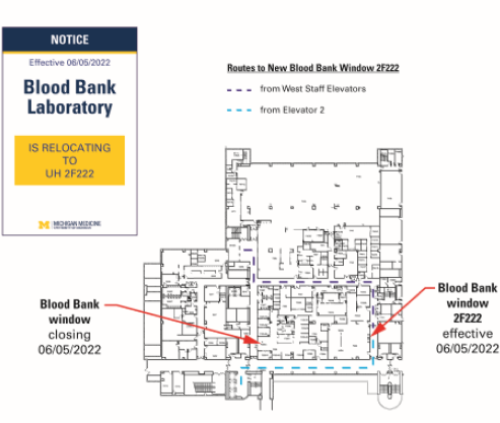
A new hallway will run north/south along the east side of the pathology spaces, allowing access to the new Blood Bank as well the new Clinical Core Laboratory. Wayfinding signs will be posted to help you find the new window and a new artwork feature of leaves around the new door frame will be added.
The Blood Bank window is used to pick up or drop off blood units or coolers of blood, drop off specimens for testing or to speak with attendings, house officers, management or techs in the Blood Bank. In addition, this is where researchers go to pick up residual specimens designated for research and expired blood units.
The Department of Pathology, in conjunction with Michigan Medicine, is in the middle of a multi-year, 50,000 sq. ft. renovation of the clinical laboratories housed in University Hospital. This renovation is focused on expanding the capabilities of the laboratories to optimize specimen throughput, enabling the laboratories to support providers and patients from Michigan Medicine, its affiliates and national clients through Michigan Medicine Laboratories outreach service (MLabs).
The newly renovated laboratories house new automation lines for chemistry and hematology, as well as state-of-the art space for other stat services.
The new Blood Bank will have modular, adaptable laboratory benches that enable the layout of the lab to change as technology evolves, additional space for the validation of new laboratory equipment, updated blood storage, optimized workflow and a separate space for the Reference Laboratory. The new RL space allows for an environment more conducive to work requiring intense focus while still allowing them to be visually connected through windows.
If you have questions regarding the relocation, please contact Terry Downs at 936-6862. For a larger graphic, click here.
Recently, the Clinical Pathology Labs at University Hospital experienced a significant milestone as part of Phase 2.3 of the Pathology Renovation and Relocation project. First, the temporary walls enclosing the old autoline space within the Clinical Core Labs were removed, with much excitement from the staff. Previously, there was a long, circular route created to move from one side of the lab to the other. This was due to the construction occurring where the old autoline had been for over 12 years.
Eric Vasbinder highlighted the changes near the new Seimens Autoline. When the new autoline was commissioned in November 2021, the old line was removed and temporary walls were put in place to allow our construction partners to renovate and upgrade the remaining portions of the Chemistry lab.
Another portion of important space was completed this week as well: the future Pathology Inventory Space (formerly known as “Path Stores"). Brooks Barnes gave a tour to Eric Vasbinder and Christine Baker to demonstrate where pallets will soon be delivered and off-loaded, as well as where the new rack system will be installed.
And finally, the new Blood Bank Laboratory was unveiled, and work began towards the lengthy process of activating the new laboratory space. Under the leadership of Dr. Robertson Davenport and Terry Downs, the Blood Bank team met to review the space and make decisions related to the upcoming activation on May 15, 2022. The work to design the new Blood Bank dates back to 2016 when the team began the process of outlining their key process flows and modeling the ideal future state. "It was rewarding and exciting to see the culmination of so many years of effort by this talented team," says Christine Baker, the Project Manager for the PRR initiative.
Last year was an eventful time within the Department of Pathology at Michigan Medicine. The continuing COVID-19 pandemic had an impact on everything from Experimental Pathology to Autopsy and Forensic medicine. As we reminisce about 2021, let's revisit some of the greatest memories.
The year started off with Department Chairman Dr. Charles Parkos' annual welcome message to students, faculty and staff, conveying positive encouragement to everyone for the big year that was to come.
Early on, the Department bid farewell to several long-time staff members who were retiring. These included Pamela Howard, Bill LeBar, Linda O'Brien, and many others.
The yearly United States and Canadian Academy of Pathology (USCAP) meeting took place in March, where several faculty members participated, albeit in virtual format. The event featured 12 live interactive microscopy courses, 37 short courses, one long course, three special topics courses, 17 evening conferences, and 31 companion society meetings. The conference also incorporated various poster sessions, live Q&A segments, a virtual exhibit hall, and many social events. Dr. Laura Lamps officially began her term as USCAP's President and impressive contributions from the likes of Drs. Joel Greenson, Sandra Camelo-Piragua, Rohit Mehra, and others, helped the Department shine.
 In April, Medical Laboratory Professionals Week (MLPW) was celebrated, with a theme of "Avengers in the Lab". Participants were involved in several fun activities including a face mask decorating competition, costume contest, virtual 5K race, lab Bingo, and much more. Efforts from Amy Drouillard, Kristina Martin, Christine Rigney, and more made the year's celebration a big success!
In April, Medical Laboratory Professionals Week (MLPW) was celebrated, with a theme of "Avengers in the Lab". Participants were involved in several fun activities including a face mask decorating competition, costume contest, virtual 5K race, lab Bingo, and much more. Efforts from Amy Drouillard, Kristina Martin, Christine Rigney, and more made the year's celebration a big success!
As springtime arrived, the Department of Pathology's Clinical Microbiology team was once again tasked with confronting the escalating needs for COVID-19 testing. As case volumes increased, the laboratory stepped up, adapted, and effectively responded to the crisis. "If it weren’t for the efforts of our pathology teams, a lot of public health officials and colleagues would have to be guessing as to how to best handle the pandemic,” said Senior Medical Technologist Christine Kizer. “We take incredible pride in what we do — and that makes it easier for us to sleep at night.”
The month of May highlighted the Department's Physician-Scientist Training Program (PSTP) as experts including Drs. Charles Parkos, Aaron Udager, Sriram Venneti, Celina Kleer, Arul Chinnaiyan, and David Lombard discussed what makes this program so unique. "The Department of Pathology is very committed to training the next generation of physician-scientists in pathology," stated Dr. Udager. "The opportunities that this program affords really exemplify our commitment to that goal."
 The summer kicked off with the second-annual Pathology Equality Walk, led by Dr. Jeffrey Myers and Medical Laboratory Scientist Jenna Koelsch. The event took place at the North Campus Research Complex in observance of the Juneteenth holiday and included over 60 faculty, staff, residents, and fellows. The walk included a trip around the perimeter of the NCRC and featured an 8-minute, 46-second kneel to honor the legacy of George Floyd.
The summer kicked off with the second-annual Pathology Equality Walk, led by Dr. Jeffrey Myers and Medical Laboratory Scientist Jenna Koelsch. The event took place at the North Campus Research Complex in observance of the Juneteenth holiday and included over 60 faculty, staff, residents, and fellows. The walk included a trip around the perimeter of the NCRC and featured an 8-minute, 46-second kneel to honor the legacy of George Floyd.
Later in June, the Department said farewell to its graduating class of Residents and Fellows. Our five graduating residents and 19 fellows moved on to exciting new career pathways within the world of Pathology. In the following month, Pathology welcomed its new class of six Residents, each from different institutions, who just arrived at Michigan Medicine. Among them were Drs. Ashley Brent, Ryan Cecchi, Elaina Daniels, Elizabeth Higginson, Amber Holtz, and Michael Olp.
At the same time, the Department said hello to a new class of Fellows and Clinical Instructors that included approximately 20 new incoming physicians training in a variety of subspecialty areas, many of whom previously completed residency training or another fellowship at Michigan Medicine. Laura Jacobus joined the education team to work closely with Marie Goldner and assist in coordinating the Residency program. Furthermore, Dr. Sean Li, along with Drs. Sara Abbott and David Manthei assumed leadership of the Residency program, succeeding Drs. Kristine Konopka and Allecia Wilson. Finally, Dr. Carol Farver departed from the institution, with Dr. Kathleen Cho being appointed as the Interim Director for the Division of Education while the search for a permanent replacement ensued.
In the heart of the summer, there was major progress made on the Pathology Renovation and Relocation (PRR) front. Here, the walls in Phase 2.2's construction area came down in order to give way to the new-and-improved Core Laboratory at the University Hospital. "The culmination of this phase of construction takes us one step closer to our collective goal of newly designed and state-of-the-art laboratories within the University Hospital to provide optimal care to our patients, explained Senior Project Manager Christine Baker. "Over the next two years, the barriers caused by space constraints will continue to come down as we move towards the completion of our project."
During September, the formation of a Pathology Anti-Racism Taskforce was announced; a new initiative dedicated to promoting equality and eliminating racism in the health system, on the Michigan campus, and within the greater community. "We are following the example of Michigan Medicine's Office of Health, Equity and Inclusion (OHEI), by organizing staff and faculty as part of our ongoing commitment to anti-racism as a strategic priority," noted Dr. Kathleen Cho.
Additionally, members from the Forensic Pathology section represented the Department at the 55th Annual Meeting of the National Association of Medical Examiners (NAME) in West Palm Beach, Florida. The seminar featured hundreds of platform and poster presentations, as well as an international forum for discussion of a broad range of issues pertaining to forensic pathology and death investigation. Residents and faculty from Michigan Medicine attended, including Drs. Allecia Wilson, Leigh Hlavaty, Lok Man Sung, Omar Rayes, Teresa Nguyen, along with many others.
September was marked by the sudden and tragic passing of Martin Lawlor, the Department's Chief Department Administrator at age 56. "I will truly miss Marty in ways that words can’t describe," expressed Dr. Charles Parkos. "I am immensely grateful for his many contributions and his friendship... I will miss him a lot.”

On October 10, the Department also hosted the yearly Fall Picnic, an in-person event at Wiard's Orchard in Ypsilanti, Michigan. Everyone from faculty to staff, to trainees, came out for a day of fun in the fall weather. Attendees participated in hayrides, pumpkin picking, visiting the petting zoo, and more. Lunch, along with cider and donuts, was served at the pavilion. Employees had the chance to mingle and connect with colleagues from all different areas of Pathology. "After what has sometimes felt like a decade of pandemic stress, it brought me such joy to see our pathology staff and their families gathering together to enjoy the beautiful day and all the fall activities that Wiard’s Orchard offers," remarked Shirley Hoffman.
As the year began to wind down, the Department released the 2021 Inside Pathology magazine, a publication that recounted the challenges and triumphs in the Department's grapple with COVID-19 in 2020. The magazine featured a number of insightful perspectives from Drs. Riccardo Valdez, Asma Nusrat, Carmen Gherasim and many more. The magazine was written, compiled, and edited by Pathology's Communications Team of Lynn McCain, Brent Temple, and Camren Clouthier.
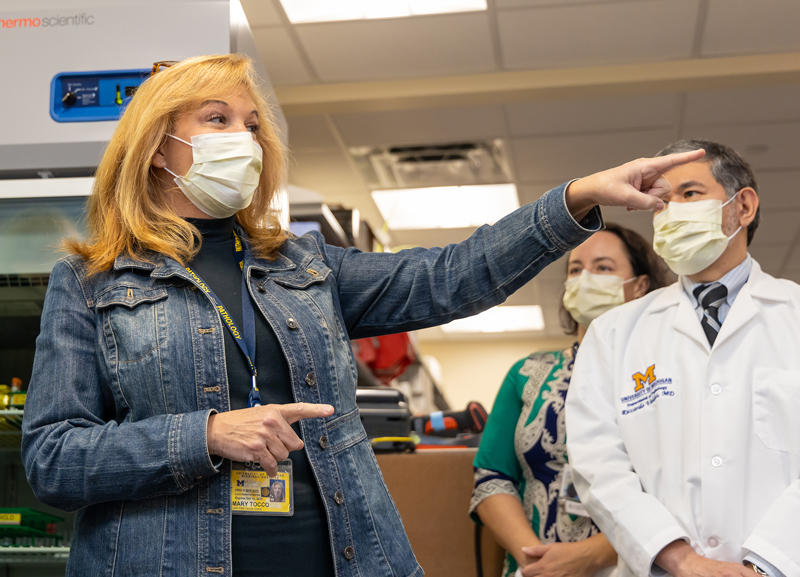
 December offered another PRR update, as the automation line at the University Hospital's Core Laboratory officially went live. Leaders from the Department received a tour from the lab team comprised of Eric Vasbinder, Mary Tocco, Todd Teifer, and Christine Baker, who guided them through the new space and offered explanations about all of the new equipment. "These automation lines are the result of years of planning, and literally, hundreds of hours spent envisioning, forecasting, designing, and training involving laboratory scientists, architects and equipment planners, engineers, project managers, IT experts, construction teams, and partnering vendors," noted Baker.
December offered another PRR update, as the automation line at the University Hospital's Core Laboratory officially went live. Leaders from the Department received a tour from the lab team comprised of Eric Vasbinder, Mary Tocco, Todd Teifer, and Christine Baker, who guided them through the new space and offered explanations about all of the new equipment. "These automation lines are the result of years of planning, and literally, hundreds of hours spent envisioning, forecasting, designing, and training involving laboratory scientists, architects and equipment planners, engineers, project managers, IT experts, construction teams, and partnering vendors," noted Baker.
Finally, the year closed with a new installment of Pathology on the Street, hosted by Kristina Martin and Christine Rigney. The video focused on COVID-19 and why people elected to get vaccinated against the virus. Later, a surge in the number of COVID-19 cases in Michigan dampened hopes of an in-person holiday celebration. However, Department leadership responded by providing boxed lunches to staff, faculty, and trainees at BSRB, UH and NCRC.
By the end of 2021, the Department had conducted 545,283 COVID diagnostic tests and 15,173 serologic (antibody) tests since the beginning of the pandemic. Approximately 275,000 of the diagnostic tests and 5,740 of the serologic tests were conducted in 2021.
Our faculty and trainees published 571 publications, received 40 new grants and processed nearly 7.4 million overall tests in the Fiscal Year 2021. The organization welcomed many new faculty and staff members and maintained its tradition of excellence in delivering outstanding patient care, conducting research, supporting educational pursuits, and combatting the challenges presented by the ongoing COVID-19 pandemic.
As the calendar flips into 2022, we would like to wish everyone a healthy and successful year here within the Department of Pathology!
With great anticipation, the UH Core Lab team hosted Department Chairman Dr. Charles Parkos and other senior leaders in our department on November 9th to demonstrate the department’s newest automation lines. These automation lines are the result of years of planning, and literally, hundreds of hours spent envisioning, forecasting, designing, and training involving laboratory scientists, architects and equipment planners, engineers, project managers, IT experts, construction teams, and partnering vendors.
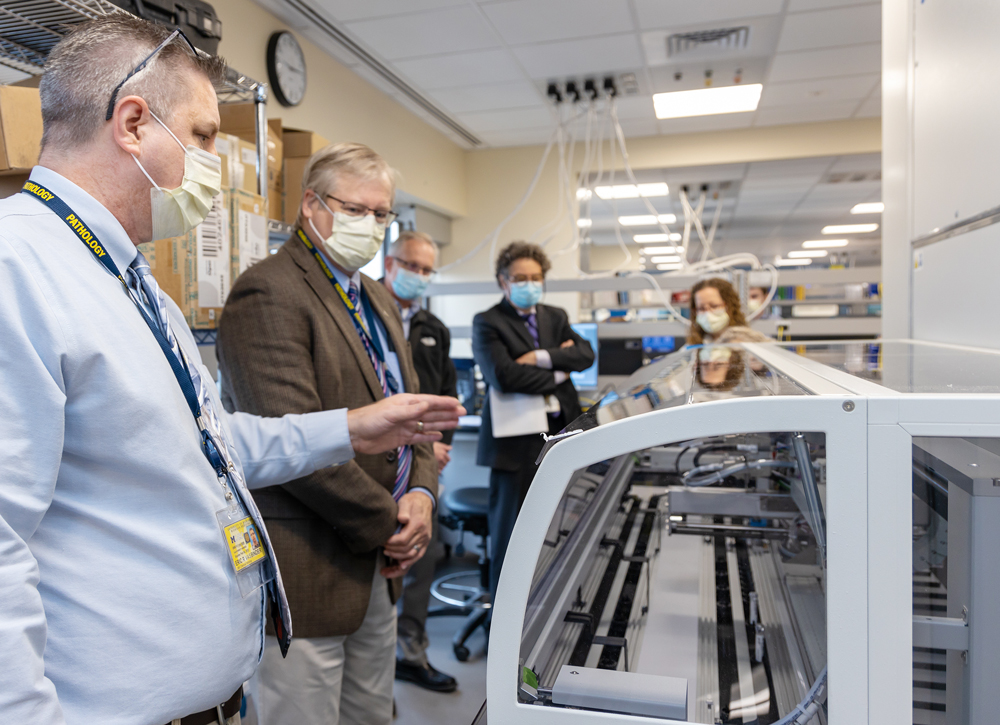 Eric Vasbinder and Todd Teifer led the team on a tour through the spaces, outlining the advantages and increased throughput that the automation is bringing to Michigan Medicine. Leadership not only got to see the complex system of automation but took turns loading some of the very first specimens to go onto the line. Mary Tocco also spoke about the upcoming pre-analytical automation components that our Department will soon add to Specimen Processing, which will further reduce turn-around times for Michigan Medicine patients.
Eric Vasbinder and Todd Teifer led the team on a tour through the spaces, outlining the advantages and increased throughput that the automation is bringing to Michigan Medicine. Leadership not only got to see the complex system of automation but took turns loading some of the very first specimens to go onto the line. Mary Tocco also spoke about the upcoming pre-analytical automation components that our Department will soon add to Specimen Processing, which will further reduce turn-around times for Michigan Medicine patients.
Speaking personally, departmental leadership mentioned the Core Lab automation lines on my first day on the job in April 2014. A week later, I sat next to Dr. Don Giachario on a short flight to a site visit and learned about his role in the department and the future visioning of an automated Core Lab. Throughout the design of the UH spaces, the automation lines featured front and center in our discussions for the ideal layout. During our lean planning exercises, we worked to envision how hematology and chemistry would align their automated capabilities for a comprehensive and integrated Core Lab. I also remember mocking this space up at a cold and dusty warehouse near the Ann Arbor airport to refine the layout.
A few years later, during the early phases of construction at UH, under the leadership of Dr. Riccardo Valdez as the Clinical Pathology Director and Janette Todd as the Clinical Core Lab manager, experts further modified the plans and added additional automated capabilities, and enhanced the layout.
 Last fall, construction crews installed the new Sysmex automation line for Hematology as part of its lab operation. In November 2020 the system officially went live, allowing the older line to be decommissioned. In February of this year, crews installed one arm of the new Siemens Chemistry line in the old Apheresis space to allow for early training and validation to run parallel to the construction effort.
Last fall, construction crews installed the new Sysmex automation line for Hematology as part of its lab operation. In November 2020 the system officially went live, allowing the older line to be decommissioned. In February of this year, crews installed one arm of the new Siemens Chemistry line in the old Apheresis space to allow for early training and validation to run parallel to the construction effort.
As soon as the contractor turned over the new spaces this past summer, truckloads of equipment started to arrive and unload at UH, starting months of installation and calibration as well as ongoing validation and training. From late October through to November 9th, years of effort culminated in various components of the automated system becoming operational.
Many thanks and appreciation to the Chemistry and Hematology teams, as well as our construction partners, IT experts, and department leadership!
 On June 12, 1987, President Ronald Reagan delivered a speech in Berlin where he famously said, “Mr. Gorbachev, tear down this wall!” These words would then be frequently used in connection to the later fall of the Berlin wall in 1989.
On June 12, 1987, President Ronald Reagan delivered a speech in Berlin where he famously said, “Mr. Gorbachev, tear down this wall!” These words would then be frequently used in connection to the later fall of the Berlin wall in 1989.
For the last 18 months, some faculty and staff may have been echoing a similar sentiment during the renovation being done in the hallways of the University Hospital. Because of construction, they have endured significantly longer routes to deliver specimens, social separation from teammates, as well as barriers, closed hallways, crowded conditions, and other challenges as result of the renovation.
However, on July 7, 2021, the walls around the Pathology Renovation and Relocation (PRR) Phase 2.2 construction areas came down. While not a world-famous event, it was nevertheless an equally inspiring sight. The department had passed another milestone as the second of five phases of construction came to an end and opening the floodgates for labs to begin activating, and moving, into the new space. On July 8, the first components of the Siemens automation line for Chemistry arrived on site. Then, on July 12, the new lab benches arrived for the teams including Chemistry, Specimen Processing, Anatomic Pathology, and Microbiology.
Over the next several weeks, Specimen Processing, the UH components of Microbiology, and the accessioning/packaging group within Anatomic Pathology will have also completed its move to their new spaces. In parallel, the automation components, including new automated Coagulation equipment, will arrive at the site, be installed and validated, and eventually start running clinical specimens.
The culmination of this phase of construction takes us one step closer to our collective goal of newly designed and state-of-the-art laboratories within the University Hospital to provide optimal care to our patients. Over the next two years, the barriers caused by space constraints will continue to come down as we move towards the completion of our project.
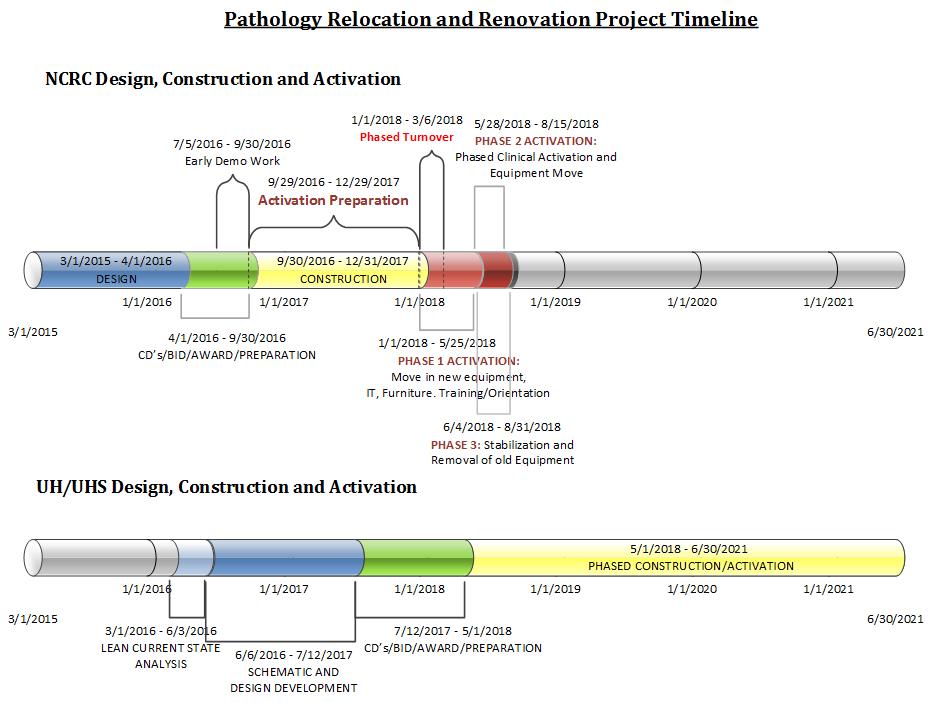
The Department of Pathology has been in its beautiful and efficient new space for [more then] ten months. Every day we learn more about the ways our work is improving due to the complex and well-thought-out design. That is the greatest success. As the clinical lead for the Pathology Renovation and Relocation (PRR) project, I have had the honor of helping to shape the future of Pathology at Michigan Medicine for the foreseeable future. Using Lean Facility Design techniques, the PRR project team facilitated the design and activation of 140,000 square feet of space at the North Campus Research Complex (NCRC), with all non-stat clinical laboratories, trainees, administration, and affiliated faculty and staff relocated over the summer of 2018. Along the way, the PRR team, of which I am a part, encountered many challenges and barriers, all of which were overcome through determination and a commitment to ensure the best possible outcomes for both patients and the department. This was a once-in-a-lifetime project for all of us and I think one of the things, in the midst of all of the challenges, that we tried to reinforce to people is that you will never have this opportunity again — to design space the way that is going to be best for the patients, the way it is going to be most efficient in accomplishing our jobs, and ultimately, provide the best level of care for our patients.
This was a once-in-a-lifetime project for all of us and I think one of the things, in the midst of all of the challenges, that we tried to reinforce to people is that you will never have this opportunity again —
Would the building be finished on time? Would we be able to get the specimens here in a timely manner and be able to track them along the way? Is our courier plan sufficiently robust? These and a myriad of other issues were at the forefront of our minds as we worked to ensure a successful relocation of the pathology laboratories to the NCRC. We spent significant amounts of time and energy to make it happen. In the end, we efficiently and safely coordinated the moves and we continue to have a very robust courier system and specimen tracking system.
To accomplish these goals, there were extensive communications and interactions between the PRR project team, the department, the campus, architects, contractors, designers, and others. We were in constant communication with them. We had regular meetings, informal face-to-face discussions, phone calls, and texts to ensure that all were on the same page, and to closely coordinate and prioritize mitigation strategies when issues were identified. In addition, the team worked closely with the department, laboratories, staff, administration, and faculty. Key to our success is that the labs were outstanding in this whole process, from leadership to staff, across the board. They excelled in organizing and articulating the validation timelines that they needed so that we could safely and efficiently coordinate the moves. The PRR team also worked closely with Metro Delivery (Ann Arbor, MI) to ensure the right schedule and the right kind of vehicles would be available to shuttle patient specimens between University Hospital and the new laboratories. Metro did a great job in accommodating all of our requests and needs. We had many unique requirements as a customer and they were very, very accommodating and helpful and made great suggestions to help us improve our processes.
 Across the department, staff have done an exceptional job in developing workflows for packaging, transporting, and tracking specimens between UH and the NCRC. Everything is happening as smoothly as possible. Everyone has done an excellent job. The Division of Quality and Healthcare Improvement (DQHI) and Pathology Informatics (PI) played a major role in this success with the development of the PathTrack asset tracking system. This critical system enables us to know where specimens are during each point in our processes.
Across the department, staff have done an exceptional job in developing workflows for packaging, transporting, and tracking specimens between UH and the NCRC. Everything is happening as smoothly as possible. Everyone has done an excellent job. The Division of Quality and Healthcare Improvement (DQHI) and Pathology Informatics (PI) played a major role in this success with the development of the PathTrack asset tracking system. This critical system enables us to know where specimens are during each point in our processes.
However, there still are challenges that have not yet been resolved. The things that have persisted are issues related to the building, and that has been a little frustrating. We are still working our way through some unanticipated issues—including adjustments and enhancements to heating and cooling as well as appropriate air-balancing and airflow. These issues were my greatest surprise in the project. The PRR Team worked hard to have success over the parts of the project for which we had direct control, but other aspects were more challenging. As it turns out, the coordination during design between the architects and engineers was not as strong as we were led to believe. This ended up causing rework and challenges during move in, some of which persist today. This was not something we anticipated or predicted, and presented a lesson the PRR team learned as we begin to tackle the next phase of the project – the UH renovation for the core labs.
Communicate often and broadly. The key takeaway from this project is that you cannot over-communicate. People hear and interpret messages in various ways. People handle change differently and as such, the messages that go out need to take different approaches to adapt to different audiences. This was a major change that had significant cultural impacts on the department. We expected that there would be an impact to our culture, but it was much more significant than we anticipated. We are working to learn from this and take that lesson into the renovation of UH, and address some of these cultural issues through communication. There is a concept from Taiichi Ohno, the father of the Toyota Production System, that states, “Having no problems is the biggest problem of all.” When “everything is fine” and remains “fine” throughout the planning process, that is an indicator that a group may not be digging deep enough and that more proactive communication is needed. Some groups are a little shyer or hesitant to share or to talk about how things are not working. So we need to be proactive in having those conversations and making sure that everyone is moving in the right direction.
The key takeaway from this project is that you cannot over-communicate.
As the UH renovation project moves forward, communication will be key to better understand challenges, to build better relationships, and to increase awareness, so that the team is not making any assumptions. That is a challenge, but also a tremendous opportunity. I appreciate the trust that the department put into me in allowing me to be in this position to help. I am proud of what we have been able to accomplish.
The newly-renovated workspace at NCRC afforded the opportunity for the department to purchase original artwork, supporting local artists. Working with Joy Naylor and Diane Bennett of Ann Arbor-based Distinct Design and U-M Interior Designer, Kate Stahl, an artwork committee chose pieces inspired by nature to complement the complex’s park-like setting.
The artists include: Francesc Burgos, Lynda Cole, Carlye Crisler, Connie Cronenwett, Kim Ensch, Karen Ehart, Helen Gotlib, Janet Kelman, Jennifer Martin, Susan Morosky, Eric Nye, Middy Potter, Elizabeth Schwartz, Jill Stefani Wagner, and Karin Wagner-Coron.
Among the artists are Art Prize winners, including Lynda Cole, whose work in oil pigment stick, cold wax, and encaustic are featured outside the chair’s office and the Division of Quality and Health Improvement. Cole, along with several other of our featured artists, is a co-owner of the WSG Gallery on Main Street in downtown Ann Arbor.
Artist, Connie Cronenwett says that she feels most like herself while she is painting and that the process gives her the opportunity to really observe. “It’s like you lose a certain part of your ego that just takes a walk and you’re so engaged with that process and it’s very challenging and it’s freeing at the same time.”
Artwork on display serves as a daily inspiration for all those who work in its midst and has inspired at least one NCRC tenant to become an artist himself, as Duane Newton has taken up watercolor lessons.
Jill Stefani Wagner uses her work as a way to document her community. ” I like to capture what life is like now. Not idealized. I always put the telephone poles and everything in because I want it to be a record,” she says. She adds that the support she has had from hospitals purchasing her art has been much appreciated and it’s a way of keeping art alive, especially after the residential market basically disappeared back in 2008. Most of the artists featured in the new space are from Ann Arbor and all are from the Midwest.
—
WSG Gallery | 306 S. Main Street, Ann Arbor, MI 48104 | Webpage
A flurry of last-minute preparations and problem solving consumed much of 2018 as the Pathology Renovation and Relocation team and strategic move captains prepared for the relocation of faculty, staff, trainees, and all the implements of a modern clinical pathology facility to the North Campus Research Complex. Throughout, the move captains ensured their laboratories, faculty neighborhood groupings, trainees, and administrative staff transitioned smoothly to Pathology’s new home 2.8 miles from the University Hospital. Over a period of approximately 3 months, these teams converged from locations across Ann Arbor into a consolidated 140,000 sq. feet state-of-the-art space designed for collaboration and to embrace the future. For the past year, the teams have been adjusting to the new space, adapting to new workflows, and taking advantage of the opportunities presented.
FIRST IMPRESSIONS
 The first thing many noticed about the new space is the natural light! Instead of being in basements or in crowded, internal laboratories without any windows, the laboratories have floor-to-ceiling walls of windows looking out at the park-like setting of the North Campus Research Complex. The space is bright and inviting. The laboratory bench space is designed to be movable, so it can be easily reconfigured as future technologies require new workflows. The labs are equipped with many familiar pieces of equipment, but also many newly-acquired pieces to enhance the capacity of the labs. Each laboratory was carefully planned using Lean Facility Design for optimal workflows and to encourage mentor/trainee interactions and teaching. In addition, the nerve centers for each lab are housed within the laboratories with clear line-of-sight between managers and the bench staff.
The first thing many noticed about the new space is the natural light! Instead of being in basements or in crowded, internal laboratories without any windows, the laboratories have floor-to-ceiling walls of windows looking out at the park-like setting of the North Campus Research Complex. The space is bright and inviting. The laboratory bench space is designed to be movable, so it can be easily reconfigured as future technologies require new workflows. The labs are equipped with many familiar pieces of equipment, but also many newly-acquired pieces to enhance the capacity of the labs. Each laboratory was carefully planned using Lean Facility Design for optimal workflows and to encourage mentor/trainee interactions and teaching. In addition, the nerve centers for each lab are housed within the laboratories with clear line-of-sight between managers and the bench staff.
Larger-than-life patient stories posted on walls in both laboratories and hallways remind all that excellent patient care is the focus of our work. Hallways and common spaces are enhanced with locally-created artwork. Conference rooms with glass walls line the exterior walls across from glass-walled offices, ensuring both offices and conference rooms are cheerfully lit. While not all offices are along this corridor, the majority are just steps away from natural light. Small offices make room for many common areas, conference rooms, and other work spaces to encourage collaboration among faculty and to enhance communication between faculty, trainees, and staff. A favorite common area to all is Central Park, complete with a long plank-wood dining table in a kitchenette adjoining high tables, soft seating, and a long fireplace, with natural greenery and artwork. This warm and welcoming space is shared by all of Pathology and is the heart of the new facility.
ADJUSTING TO CHANGE
 The beautiful facilities provide the framework for success, yet they also require staff to adapt to the new environments. In the molecular pathology division, six laboratories that were scattered across Ann Arbor, each with separate cultures and norms, are now co-located in contiguous molecular laboratories. The new space provides an opportunity to have back-up equipment available in case of equipment failure. “The move is a win for the Molecular Division,” stated Dr. Thomas Giordano, Director of the Division of Molecular Pathology. “We were in Traverwood (an off-site facility),” stated Dr. Lina Shao, Director of Cytogenetics, “which was isolating. Now we are at the NCRC and are more fully integrated. We feel like we are a real part of the Department. The move had a positive impact for our lab.”
The beautiful facilities provide the framework for success, yet they also require staff to adapt to the new environments. In the molecular pathology division, six laboratories that were scattered across Ann Arbor, each with separate cultures and norms, are now co-located in contiguous molecular laboratories. The new space provides an opportunity to have back-up equipment available in case of equipment failure. “The move is a win for the Molecular Division,” stated Dr. Thomas Giordano, Director of the Division of Molecular Pathology. “We were in Traverwood (an off-site facility),” stated Dr. Lina Shao, Director of Cytogenetics, “which was isolating. Now we are at the NCRC and are more fully integrated. We feel like we are a real part of the Department. The move had a positive impact for our lab.”
The anatomic pathology laboratories now require patient specimens be transported between the UH and NCRC. This created an entirely new workflow, requiring additional staff, and a complex specimen tracking process. Pathology Informatics and the Division of Quality and Healthcare Improvement elegantly solved the tracking challenges with PathTrack™, which was featured in last year’s edition of Inside Pathology Magazine. “When we first moved in, PathTrack wasn’t able to keep up with the increased demand, so the application did not work efficiently as the number of users increased,” explained Dr. Ul Balis, Director of Pathology Informatics. “So the team stepped up, not only solving that architectural problem, but also extending certain features. Now we are deploying PathTrack to multiple clinical sites at the University Hospital and the Taubman clinic.” PathTrack has attracted significant attention from other organizations as well.
Administrative staff are located in close proximity to the faculty providing more opportunities for interaction and discussion, improved communication and engagement.
 With the more open and collaborative environments, faculty and staff also faced adjustments. Administrative staff are located in close proximity to the faculty providing more opportunities for interaction and discussion, improved communication and engagement. Faculty are now part of multi-disciplinary neighborhoods, which has led to opportunities to reach out to neighbors for quick case conferences or for impromptu meetings at multi-headed microscopes. Residents and fellows are located in bright, modern space at the heart of the laboratories, adjacent to the sign-out areas and near the faculty suite. Robust educational experiences were built into the layout of the laboratories and sign out areas. While the overall environment for our trainees significantly improved, the relocation also meant that the residents and fellows needed to commute between the hospital and the laboratories for rotations in the stat labs and to attend some seminars and multi-disciplinary conferences. Digital signage prominently displayed throughout the space includes both inbound and outbound bus arrival times to assist in this commute. Pathology Informatics is located just down the hall from the faculty suite and administrative offices, which enhances service delivery and access for technical support. “Having MLabs right here with us makes it much easier to reach out to the outreach team themselves,” said Dr. David McClintock, Associate Professor of Pathology Informatics and Assistant CIO for Michigan Medicine. “We are close to the billing team and both AP and CP operations as well as Administration,” added Kathy Davis, Administrative Director of Pathology Informatics.
With the more open and collaborative environments, faculty and staff also faced adjustments. Administrative staff are located in close proximity to the faculty providing more opportunities for interaction and discussion, improved communication and engagement. Faculty are now part of multi-disciplinary neighborhoods, which has led to opportunities to reach out to neighbors for quick case conferences or for impromptu meetings at multi-headed microscopes. Residents and fellows are located in bright, modern space at the heart of the laboratories, adjacent to the sign-out areas and near the faculty suite. Robust educational experiences were built into the layout of the laboratories and sign out areas. While the overall environment for our trainees significantly improved, the relocation also meant that the residents and fellows needed to commute between the hospital and the laboratories for rotations in the stat labs and to attend some seminars and multi-disciplinary conferences. Digital signage prominently displayed throughout the space includes both inbound and outbound bus arrival times to assist in this commute. Pathology Informatics is located just down the hall from the faculty suite and administrative offices, which enhances service delivery and access for technical support. “Having MLabs right here with us makes it much easier to reach out to the outreach team themselves,” said Dr. David McClintock, Associate Professor of Pathology Informatics and Assistant CIO for Michigan Medicine. “We are close to the billing team and both AP and CP operations as well as Administration,” added Kathy Davis, Administrative Director of Pathology Informatics.
BUILDING ON SUCCESS
Now that we have been at the NCRC for one year, people are settling into their new space and routines and are beginning to look to how they can take full advantage of our facilities.
“The molecular laboratories have come together and the changes we have seen with the molecular lab and our work are significant,” stated Dr. Shao. “In cytogenetics, we were manually extracting DNA. The molecular lab, however, uses robots to do DNA extractions. Now we are able to use their resources. We validated DNA extraction by robots for both blood and bone marrow. That saves us a lot of work.” In addition, the new microarray laboratory layout allowed for other efficiencies. Rather than being in rooms on opposite ends of the hallway, the pre-PCR and post-PCR rooms are now in adjacent air-pressure-controlled environments to reduce contamination possibilities. Technologists simply move specimens a few steps rather than boxing them up and walking down the hall. Use of a new Thermotron eliminated the need for a cold room to process specimens, reducing exposure to caustic chemicals. Specimens are now safely processed in the contained, vented, box-like Thermotron.
“Now that we have the move done,” stated Dr. McClintock, “we are starting to work on new projects. We have some very good potential pathology solutions in the pipeline that this lab has enabled us to do. We have new, dedicated space for development for the future.” “This new space allowed us to be more productive with the precision medicine project,” agreed Dr. Balis. “One example of this is the whole slide-viewer technology developed by Dr. Jerome Chang, which has become the national standard now for the NCI/NIDDK for viewing whole slide images. That was a huge win!”
As Pathology continues to integrate within the new space and adjust to new possibilities, a new project has been initiated – the renovation of the STAT and core laboratories at the University Hospital. This four-year project will continue to both challenge us and help us improve patient care as we look to the future. The PRR team learned a great deal from the relocation of our laboratories to the NCRC. Many of these lessons learned are being applied to the University Hospital Project. We are looking forward to the possibilities for enhanced patient care that will emerge as a result of these renovations.
 ON THE COVER
ON THE COVER
Breast team reviewing a patient's slide. (From left to right) Ghassan Allo, Fellow; Laura Walters, Clinical Lecturer; Celina Kleer, Professor. See Article |
newsletter
INSIDE PATHOLOGYAbout Our NewsletterInside Pathology is an newsletter published by the Chairman's Office to bring news and updates from inside the department's research and to become familiar with those leading it. It is our hope that those who read it will enjoy hearing about those new and familiar, and perhaps help in furthering our research. CONTENTS
|
 ON THE COVER
ON THE COVER
Autopsy Technician draws blood while working in the Wayne County morgue. See Article |
newsletter
INSIDE PATHOLOGYAbout Our NewsletterInside Pathology is an newsletter published by the Chairman's Office to bring news and updates from inside the department's research and to become familiar with those leading it. It is our hope that those who read it will enjoy hearing about those new and familiar, and perhaps help in furthering our research. CONTENTS
|
 ON THE COVER
ON THE COVER
Dr. Sriram Venneti, MD, PhD and Postdoctoral Fellow, Chan Chung, PhD investigate pediatric brain cancer. See Article |
newsletter
INSIDE PATHOLOGYAbout Our NewsletterInside Pathology is an newsletter published by the Chairman's Office to bring news and updates from inside the department's research and to become familiar with those leading it. It is our hope that those who read it will enjoy hearing about those new and familiar, and perhaps help in furthering our research. CONTENTS
|
 ON THE COVER
ON THE COVER
Director of the Neuropathology Fellowship, Dr. Sandra Camelo-Piragua serves on the Patient and Family Advisory Council. |
newsletter
INSIDE PATHOLOGYAbout Our NewsletterInside Pathology is an newsletter published by the Chairman's Office to bring news and updates from inside the department's research and to become familiar with those leading it. It is our hope that those who read it will enjoy hearing about those new and familiar, and perhaps help in furthering our research. CONTENTS
|
 ON THE COVER
ON THE COVER
Residents Ashley Bradt (left) and William Perry work at a multi-headed scope in our new facility. |
newsletter
INSIDE PATHOLOGYAbout Our NewsletterInside Pathology is an newsletter published by the Chairman's Office to bring news and updates from inside the department's research and to become familiar with those leading it. It is our hope that those who read it will enjoy hearing about those new and familiar, and perhaps help in furthering our research. CONTENTS
|
 ON THE COVER
ON THE COVER
Dr. Kristine Konopka (right) instructing residents while using a multi-headed microscope. |
newsletter
INSIDE PATHOLOGYAbout Our NewsletterInside Pathology is an newsletter published by the Chairman's Office to bring news and updates from inside the department's research and to become familiar with those leading it. It is our hope that those who read it will enjoy hearing about those new and familiar, and perhaps help in furthering our research. CONTENTS
|
 ON THE COVER
ON THE COVER
Patient specimens poised for COVID-19 PCR testing. |
newsletter
INSIDE PATHOLOGYAbout Our NewsletterInside Pathology is an newsletter published by the Chairman's Office to bring news and updates from inside the department's research and to become familiar with those leading it. It is our hope that those who read it will enjoy hearing about those new and familiar, and perhaps help in furthering our research. CONTENTS
|
 ON THE COVER
ON THE COVER
Dr. Pantanowitz demonstrates using machine learning in analyzing slides. |
newsletter
INSIDE PATHOLOGYAbout Our NewsletterInside Pathology is an newsletter published by the Chairman's Office to bring news and updates from inside the department's research and to become familiar with those leading it. It is our hope that those who read it will enjoy hearing about those new and familiar, and perhaps help in furthering our research. CONTENTS
|
 ON THE COVER
ON THE COVER
(Left to Right) Drs. Angela Wu, Laura Lamps, and Maria Westerhoff. |
newsletter
INSIDE PATHOLOGYAbout Our NewsletterInside Pathology is an newsletter published by the Chairman's Office to bring news and updates from inside the department's research and to become familiar with those leading it. It is our hope that those who read it will enjoy hearing about those new and familiar, and perhaps help in furthering our research. CONTENTS
|
 ON THE COVER
ON THE COVER
Illustration representing the various machines and processing used within our labs. |
newsletter
INSIDE PATHOLOGYAbout Our NewsletterInside Pathology is an newsletter published by the Chairman's Office to bring news and updates from inside the department's research and to become familiar with those leading it. It is our hope that those who read it will enjoy hearing about those new and familiar, and perhaps help in furthering our research. CONTENTS
|
 ON THE COVER
ON THE COVER
Rendering of the D. Dan and Betty Khn Health Care Pavilion. Credit: HOK |
newsletter
INSIDE PATHOLOGYAbout Our NewsletterInside Pathology is an newsletter published by the Chairman's Office to bring news and updates from inside the department's research and to become familiar with those leading it. It is our hope that those who read it will enjoy hearing about those new and familiar, and perhaps help in furthering our research. CONTENTS
|
MLabs, established in 1985, functions as a portal to provide pathologists, hospitals. and other reference laboratories access to the faculty, staff and laboratories of the University of Michigan Health System’s Department of Pathology. MLabs is a recognized leader for advanced molecular diagnostic testing, helpful consultants and exceptional customer service.